Dermoid Cyst Definition: a benign congenital cyst in the orbit lined by squamous epithelium and containing adnexal structures in the wall.
Incidence/Prevalence: Dermoid cysts make up between 4-15% of orbital tumors in most series. The lesions are present at birth but may become manifest later in childhood or even adulthood.
Etiology: Dermoid cysts are believed to arise as embryonic epithelial nests that become entrapped during embryogenesis and pinched at suture lines of bones.
Clinical Findings: On clinical grounds dermoid cysts can be divided into superficial and deep masses.
Superficial dermoid cysts are usually situated temporally, and present as painless, firm, 1-2 cm diameter, immobile masses that are noticed during infancy and originate most commonly from the frontozygomatic suture or frontolacrimal suture.
Deep dermoid cysts often present as slow growing masses in later childhood or adulthood and can arise from any suture of the orbit, but most commonly the frontozygomatic. Deep dermoid cysts may protrude through the frontozygomatic suture to take a dumbbell shape. Involvement of sutures on the ethmoid bone, or area around the superior orbital fissure have been reported. The patients present with symptoms and signs referable to the mass effect in the orbit (proptosis, bulging upper eyelid, downward (or upward) displacement of the eye), visual and ocular motor defects, etc. Ruptured dermoid cysts may present as draining fistulas.
Radiologic Findings:Superficial dermoids are round masses that contain a lucent center (fat or muscle density) and are generally not associated with a defect in the bone.
Deep dermoid cysts are often accompanied by bone defects at the suture. For example, the classic dumbbell shaped lesion may extend thru the frontozygomatic suture into the temporalis fossa. There may be calcification, or an area where adjacent bone is smoothly disrupted.
Histopathology: 
Histologically, dermoid cysts contain desquamated squamous epithelium and keratin in the lumen (arrow 1) and are encapsulated and lined by keratinized stratified squamous epithelium (arrows 2 and 3). A key for the diagnosis is the presence of adnexal structures including sebaceous glands (arrows 2 and 4 here)
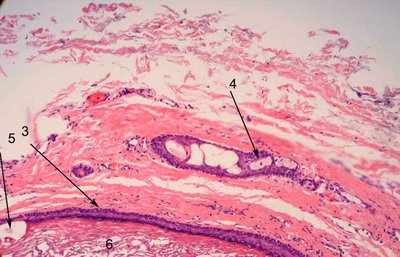
. Hair roots, sweat glands, apocrine glands and lacrimal glands may also appear in the wall of the cyst. Higher magnification shows that the lumen contains hair shafts and keratin (arrows 5 and 6, respectively). Polarization of the sections will often highlight the hair shafts in the lumen.
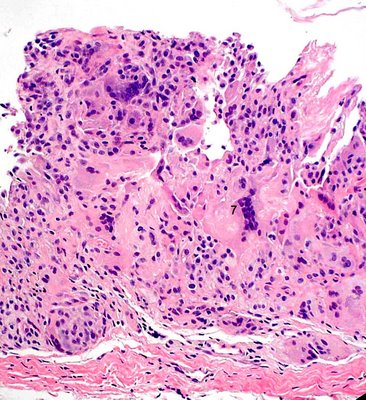
If the wall does not bear adnexal structures, the term epidermal or keratin cyst is applied. Intraorbital cysts may also be lined by respiratory epithelium or conjunctival epithelium. Rupture of cyst contents may produce a marked granulomatous reaction and the residual cyst that forms may have its squamous epithelial lining completely replaced by epithelioid histiocytes and multinucleated giant cells (number 7 below).
Most ruptured cysts occur between the
ages of 20-40 and some authors note a relationship between the volume of the cyst (2197 cubic) and the likelihood of finding a hidden rupture (
see reference).
Treatment:Superficial dermoids are often removed before the 5th year of life to avoid traumatic rupture and some authors recommend surgery by the age of 3-4.
Deep dermoids may be very difficult to remove and require careful preoperative assessment of the anatomic structures involved. It is important to attempt removal of the cyst intact and to remove the entire lining. Lesions may extend into the intracranial cavity severely complicating and compromising the attempts to remove them.
Prognosis: Superficial dermoids are generally quite easily handled with little morbidity. Deep dermoids involving complicated orbital structures or extending in the intracranial cavity are prone to complications from either rupture during removal or damage to adjacent structures. A team approach with other services may be necessary.
References:Dithmar et al. Klin Monatsbl Augenheilkd. 1993 Covered rupture of periocular dermoid cysts.
