Seborrheic keratosisDefinition: benign neoplasm of the epidermis in which keratinocytes in G1 arrest are accumulated. The epithelial proliferation of the skin characterized by a stuck on appearance clinically and acanthosis and papillomatosis pathologically.
Incidence/Prevalence: the most common eyelid lesion in our surgical material accounting for more than half of all biopsies.
Etiology: There is evidence that P16, a cyclin-dependent kinase inhibitor, has a role in the etiology of the seborrheic keratosis. P16 is expressed in all of the cells of seborrheic keratoses, whereas normal keratinocytes expressed p16 only in the granular cells. Other factors such as cyclins A, D and E, p21, p53, Rb gene product, and TP1, are not expressed in SK cells.
Clinical Findings: Seborrheic keratoses occur most commonly in middle age and older individuals. They are often, oval, dome-shaped or verrucous and have a “stuck-on” appearance and vary in color from pink to brown. The lesion may range greatly in size from millimeters to centimeters. Irritated seborrheic keratosis, has been called inverted follicular keratosis. Most lesions are recognized easily clinically but many are often misdiagnosed as keratoacanthoma, basal carcinoma, actinic keratosis and even malignant melanoma (when they are pigmented). Squamous carcinoma in situ has been reported as a combined lesion in seborrheic keratosis. Sudden onset of multiple seborrheic keratoses is known as the Leser-Trélat sign and is associated with adenocarcinoma of the colon. The keratoses in this case may be part of an evolving acanthosis nigricans.
Histopathology: Histopathologically, several architectural patterns are described. The criteria used in the diagnosis are hyperkeratosis (very slight in the figure), acanthosis (arrow 1), and some degree of papillomatosis (the undulating epithelial infoldings at arrow 2 in the figure).
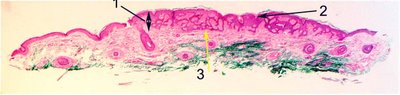
Acanthosis, thickening of the epithelium (arrow 1) may take the form of proliferation of epithelium in interwoven or reticular tracts of epithelium (arrow 3), as abundant pseudohorned cysts, as a nested clonal pattern, as a hyperkeratotic pattern, and as a verrucous proliferation.
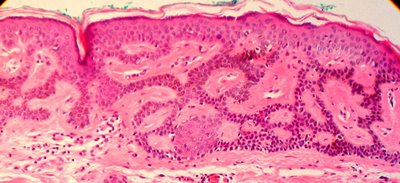
The subdivision of the type of seborrheic keratosis has value only in the recognition of the broad range of appearances. Illustrated here is the reticular or adenoid type with double rows of epithelium (yellow arrow 3 in first image). A characteristic finding in most types of seborrheic keratoses is the formation of pseudohorn cysts, which is the appearance of concentrically laminated collections of surface keratin within the acanthotic epithelium. The pseudohorn cyst is nothing more than a section of invaginated keratinizing epithelium. Increased pigmentation may be seen on the basal layer of the epidermis probably due to melanin uptake by keratinocytes. The dark brown color of an otherwise typical seborrheic keratosis, may then be confused clinically with malignant melanoma. Many pathologists do not distinguish between squamous papilloma and seborrheic keratosis because the seborrheic keratoses exhibit papillomatosis in some areas that is indistinguishable from squamous papilloma and vice versa. In the illustration below one sees what was clinically a squamous papilloma (notice the base of the lesion is arrow 5 and the distinctive polypoid shape).

Clearly the lesion features papillomatosis (arrow 4) and interwoven epithelial expansion typical of seborrheic keratosis (arrow 6). In yet another example of a clinical "squamous papilloma", there is clear evidence of a polypoid lesion (arrow 5 shows the base of the lesion) and the typical interwoven epithelial pattern characteristic of a seborrheic keratosis. This lesion even features pseudohorn cysts (arrow 7) a classic feature of the seborrheic keratosis.

There seems to be little merit in separating the squamous papilloma and seborrheic keratosis in pathologic classification until or unless a clear etiologic difference is determined.
Treatment: Simple excision is often performed for diagnosis, cosmetic reasons and if the patient is irritated by the neoplasms. All specimens should be sent from histopathology as misdiagnoses abound. The all too frequent practice of discarding the lesion to save money from the histopathological analysis is essentially indefensible when a recurrent lesion in the same area proves to be a malignant melanoma years later. If the patient has the sudden onset of multiple lesions, referral for colonoscopy is indicated.
Reference: Nakamura, S. British Journal Dermatology 2003:149:560.
