Acanthamoeba Keratitis
Definition: Acanthamoeba protozoa most commonly cause infection in soft contact lens wearers who do not take appropriate precautions in cleaning and sterilizing their lenses.
Incidence/ Prevalence: A dramatic rise in incidence occurred in the 1980s with contact lens wear. Estimates of incidence are about 1.4 cases/million population each year.(Ref 1)
Etiology: Acanthamoeba is a free-living genus of amoeba that is essentially ubiquitous in the freshwater, seawater, and air. The most frequently involved species are A castellani and A polyphagia.
Clinical Findings: Patients presenting with Acanthamoeba keratitis usually have severe eye pain, and a ring infiltrate. The infiltrate may have a dendritiform pattern that is confused with herpetic lesions. Special culture techniques and media, including nonnutrient blood agar layered with E coli, are required to grow Acanthamoeba. For a link to a clinical photograph click here.
Gross findings: Under the dissecting microscope the cornea will reveal a dense stromal infiltrate and occasionally the density of organisms is great enough for one to see numerous cysts. 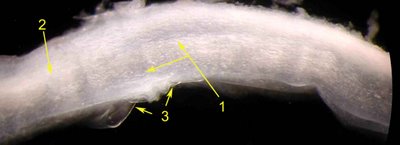 In the image shown cystic structures are provocative (arrow number 1) that correlated with the microscopic findings. In addition one can see ulceration of the surface and a very dense stromal infiltrate (arrow 2) that blurs the lamellar organization of the cornea. One appreciates the magnification of the dissecting microsope as one recognizes Descemet's membrane (arrow 3).
In the image shown cystic structures are provocative (arrow number 1) that correlated with the microscopic findings. In addition one can see ulceration of the surface and a very dense stromal infiltrate (arrow 2) that blurs the lamellar organization of the cornea. One appreciates the magnification of the dissecting microsope as one recognizes Descemet's membrane (arrow 3).
Histopathology: In most cases sections show a background of necrotizing keratitis with an interlamellar necrotic infiltrate. However, there may be little inflammation. As shown in the image with the bright arrow the organisms have a double walled cyst in microscopic sections that is characteristic. The organisms are quite visible with hematoxylin and eosin stained sections and are accentuated by PAS (see figure).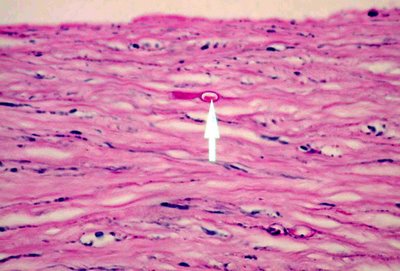 Note the necrotic lamellae, keratocyte and lymphocyte nuclei in the corneal stroma. Other techniques, such as the use of monoclonal antibodies, may provide confirmation of the species for cysts and trophozoites in tissue sections.
Note the necrotic lamellae, keratocyte and lymphocyte nuclei in the corneal stroma. Other techniques, such as the use of monoclonal antibodies, may provide confirmation of the species for cysts and trophozoites in tissue sections. 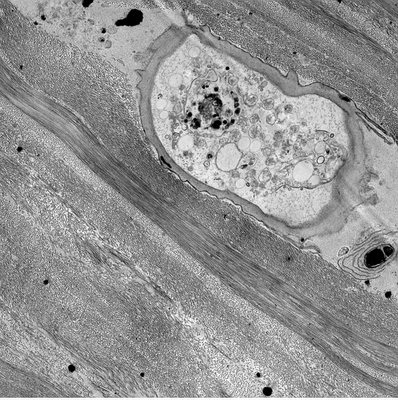 Electron microscopy beautifully demonstrates the morphologic features of the microbe but is unnecessary for diagnosis.
Electron microscopy beautifully demonstrates the morphologic features of the microbe but is unnecessary for diagnosis.
Air dried Geimsa stained smears or scraping of the cornea epithelium dramatically feature the organism with a cystic outerwall, a central contractile vacuole and single small nucleus and prominent nucleolus.  Click to enlarge the photographic image below.
Click to enlarge the photographic image below.
This is a MGG stained cytology smear of a scraping from the corneal epithelium, the organism(arrow) is slightly larger than the epithelial cells and show a distinct cell wall but a much smaller nucleus. The cytoplasm is markedly vacuolated, and there is the very distinctive central contractile vacuole used to pump water in and out of the cell. These features are very distinct from the other cells. Photograph original magnification x 400.
Treatment: A variety of topically applied therapeutic agents alone or in combination have been effectively used, including propamidine isethionate, clotrimazole, polyhexamethylene biguanide, and chlorhexidine. Penetrating keratoplasty is best reserved to restore vision after the acute infection has been effectively treated.
Reference:
1. Radford et al BJO 1998 82:1382.
2. Illingworth CD, Cook SD: Acanthamoeba keratitis. Surv Ophthalmol. 1998 May-Jun;42(6):493-508. Review
